My child still wets the bed—should I be worried?
A story told freely—based on patient accounts
I wake up and notice it right away.
I haven't even moved yet, but I already know.
The bed is wet.
I don't do it on purpose.
I don't understand why it happens.
I just want it to stop.

AI-generated image of a child suffering from nocturnal enuresis.
This story is fictional—but it is based on a real patient from my practice.
This girl is 9 years old.
And she didn't come to see me because of bedwetting.
But because of an open bite.

clinical presentation of an anterior open bite
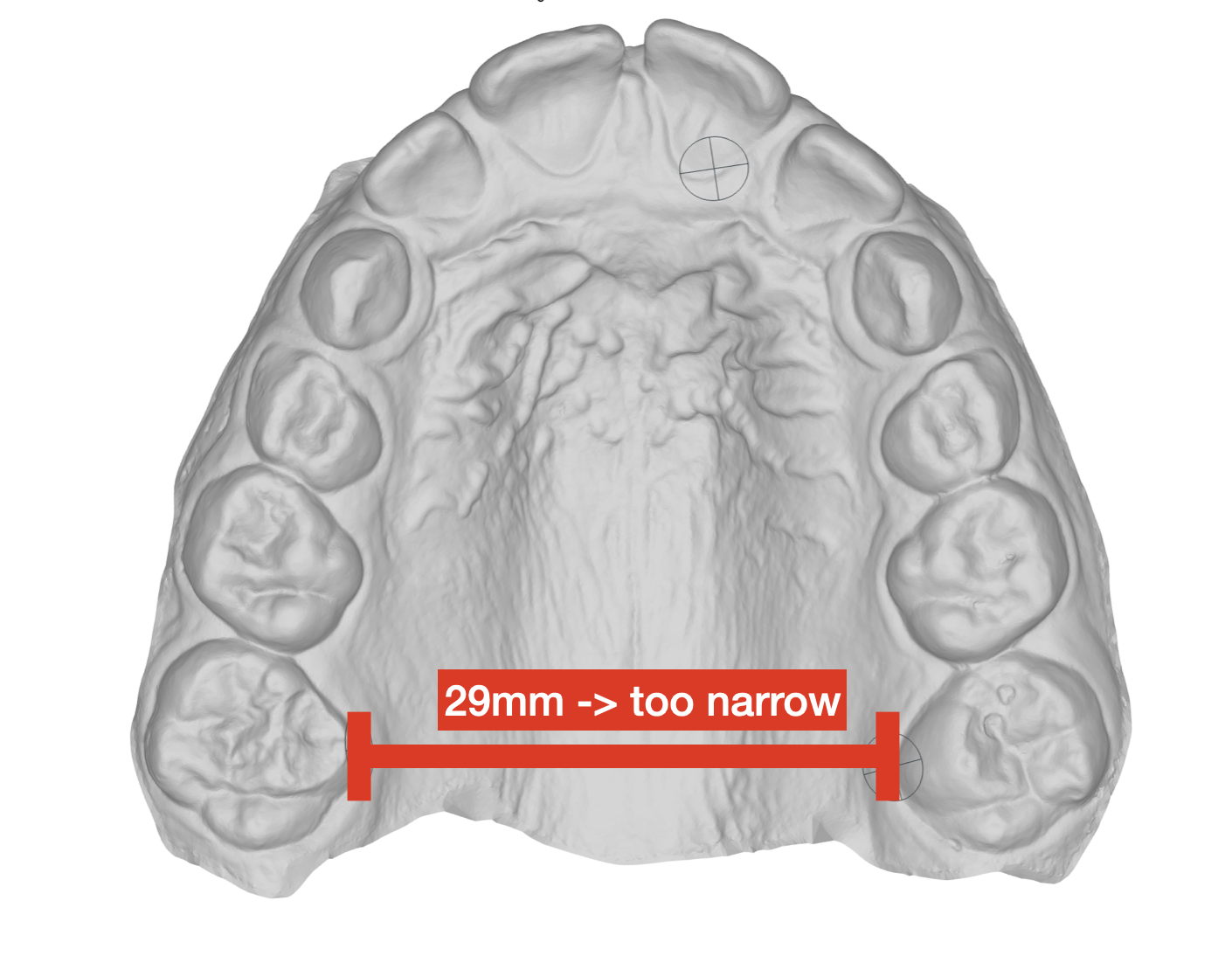
What we saw during the examination
The clinical examination and the evaluation of the pediatric sleep questionnaire revealed a clear picture:
Mouth breathing
Snoring
Restless sleep
Occasional bedwetting
Narrow upper jaw
Not enough space for the tongue, resulting in an open bite
The tongue simply didn't have room where it was supposed to be:at the top of the palate.
Instead, it lay deep in her mouth or was clenched between her teeth.
Why a tongue-tie is NOT the solution here
In such cases, a so-calledtongue guardis often used.
The idea is to prevent the tongue from resting between the teeth.
The problem with that is:
Although the tongue is "held back"—
—it still hasnowhere to rest properly.
This means:
The cause remains
The tongue cannot find a stable resting position
The functional problems (breathing, swallowing, growth) remain unchanged
A tongue scraper, therefore, treats thesymptom, not thecause.
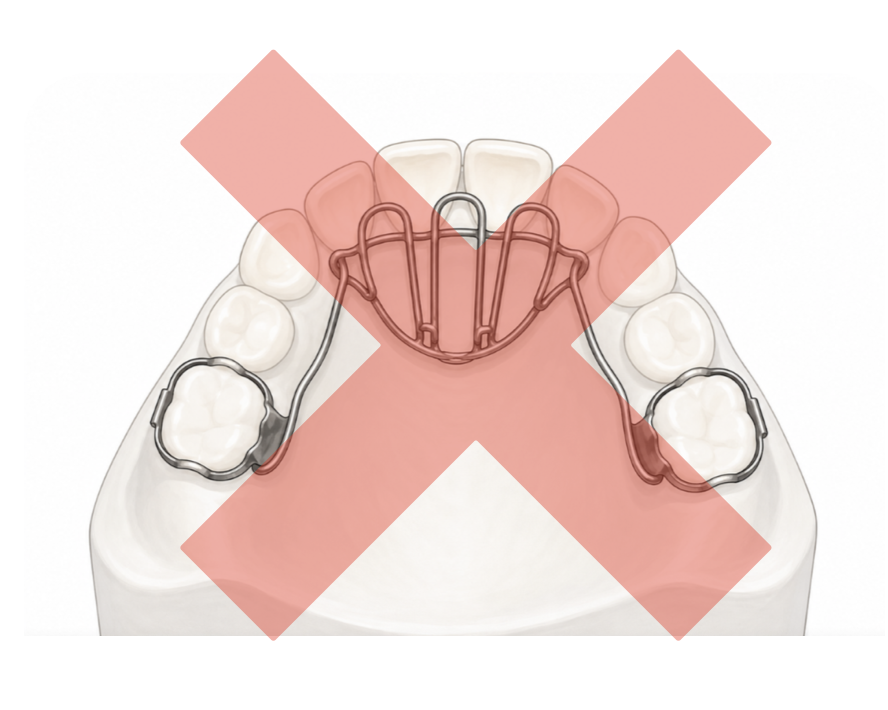
A tongue guard isn't the right solution here
The key approach: making room instead of blocking
This patient had already undergone an ENT examination:
No enlarged tonsils or adenoids; no need for surgery.
Our focus was therefore on function and anatomy.
Treatment:
Upper jaw expansion
as a result: more room for the tongue
Improvednasal breathing, especially during sleep
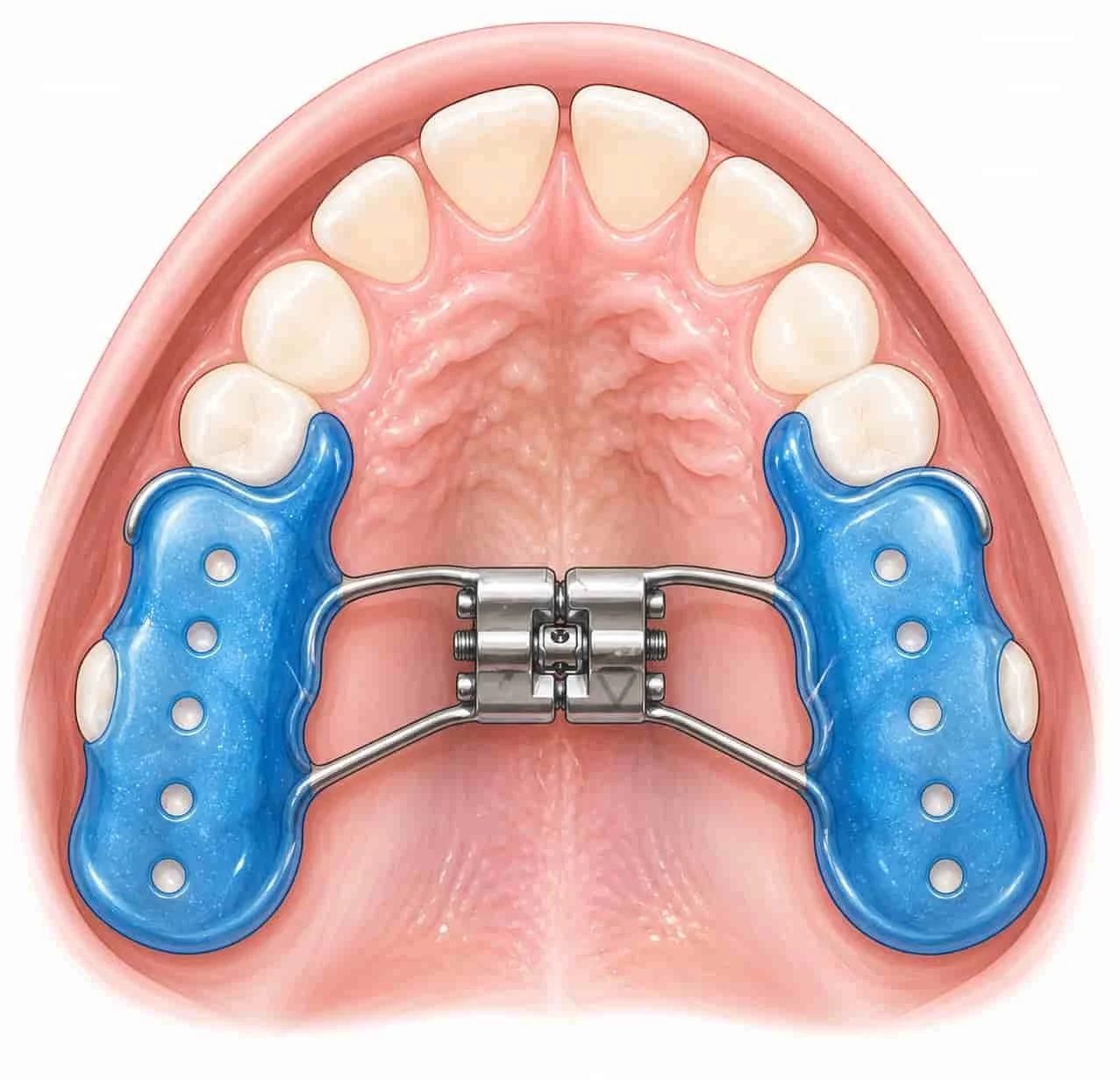
Cap plate for maxillary expansion and expansion of the nasal floor

The open bite closed on its own after the maxillary expansion—without the need for a tongue barrier.
What happened next
Over time, something very exciting became apparent:
Nasal breathingbecame calmer and more steady
Sleepbecame much more restful
Thebite closedon its own—without a tongue guard
And:
Thebedwetting stopped completely

An AI-generated image of a girl who is happy and carefree.
Why these things are connected
One factor that is often overlooked when it comes to bedwetting issleep quality.
Children who:
have trouble breathing
breathe through your mouth
or sleep very restlessly
often have adeeper, less regulated sleep.
They “don’t wake up in time” when they feel the urge to urinate.
Not because they don’t want to—but because their bodies aren’t functioning optimally.

Mouth breathing can lead to a dry mouth, reduced saliva production (and thus an increased risk of tooth decay), and snoring
Other possible causes of bedwetting
Of course, there are other reasons as well:
Delayed development of bladder control
Genetic factors
Hormonal Regulation (ADH)
Stress or emotional strain
Very deep sleep (regardless of breathing)
👉 It’s always important to take aholistic view.
At what age should a child be potty-trained at night?
Most children develop nighttime bladder control between the ages of 5 and 7.
Bedwetting after the age of 7 is:
quite often
but a sign that one should take a closer look
The Often Overlooked Connection: Sleep & Breathing
When it comes to bedwetting, many parents first think of the bladder.
But in many cases, the cause liesone level deeper:
during sleep
and while breathing

An AI-generated image of the girl from the story, happily enjoying a sleepover