What is right for me: MARPE, MSE, DOME, MASPE, RPE, SARPE, … ?
Many different names circulate for one and the same treatment: MARPE, MSE, DOME, MASPE. This can be quite confusing – not only for patients but also for colleagues. The reason for this is that each practitioner has their own philosophy for maxillary expansion.
Here is a brief explanation of the acronyms:
MARPE: Mini-Implant Assisted Rapid Palatal Expansion
MASPE: Mini-Implant Assisted Slow Palatal Expansion
MSE: Maxillary Skeletal Expansion
DOME: Distraction Osteogenesis Maxillary Expansion
What they all have in common: the goal of skeletally expanding the upper jaw and not just widening the dental arch.
Skeletal Upper Jaw Expansion with a Mini-Implant Supported Expander
Previously, bony expansion of the upper jaw was only possible in children because their bone sutures had not yet fused.
Since the invention of mini-implants, this orthopedic expansion of the maxilla is also possible for adolescents and adults – entirely without jaw surgery.
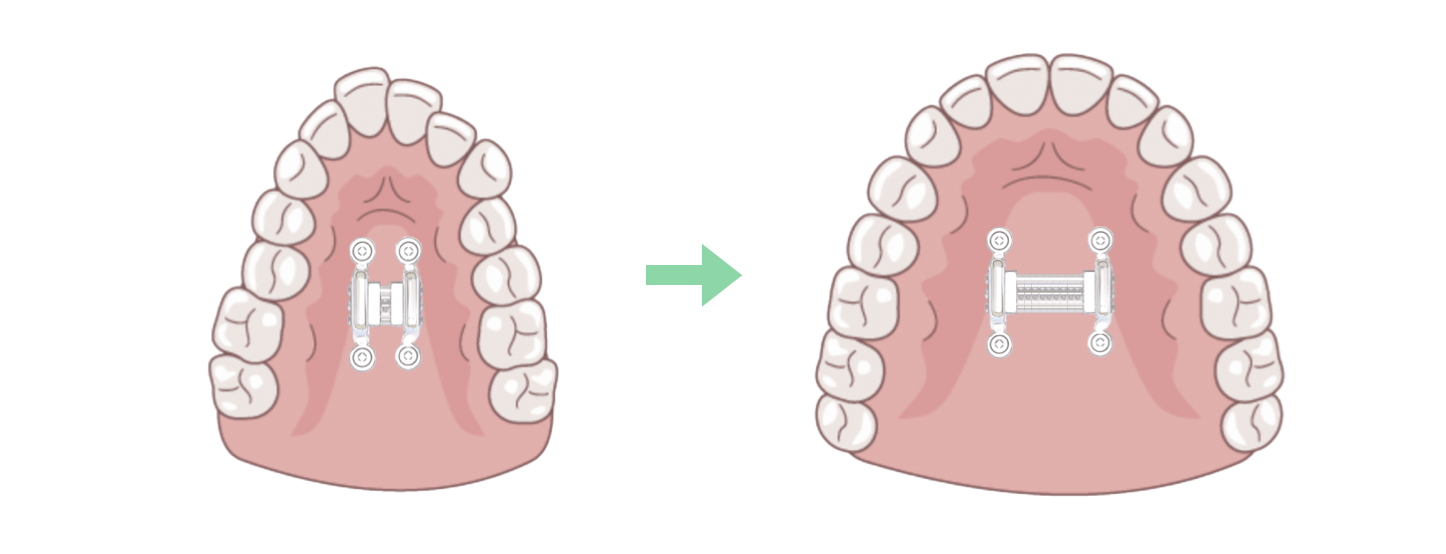
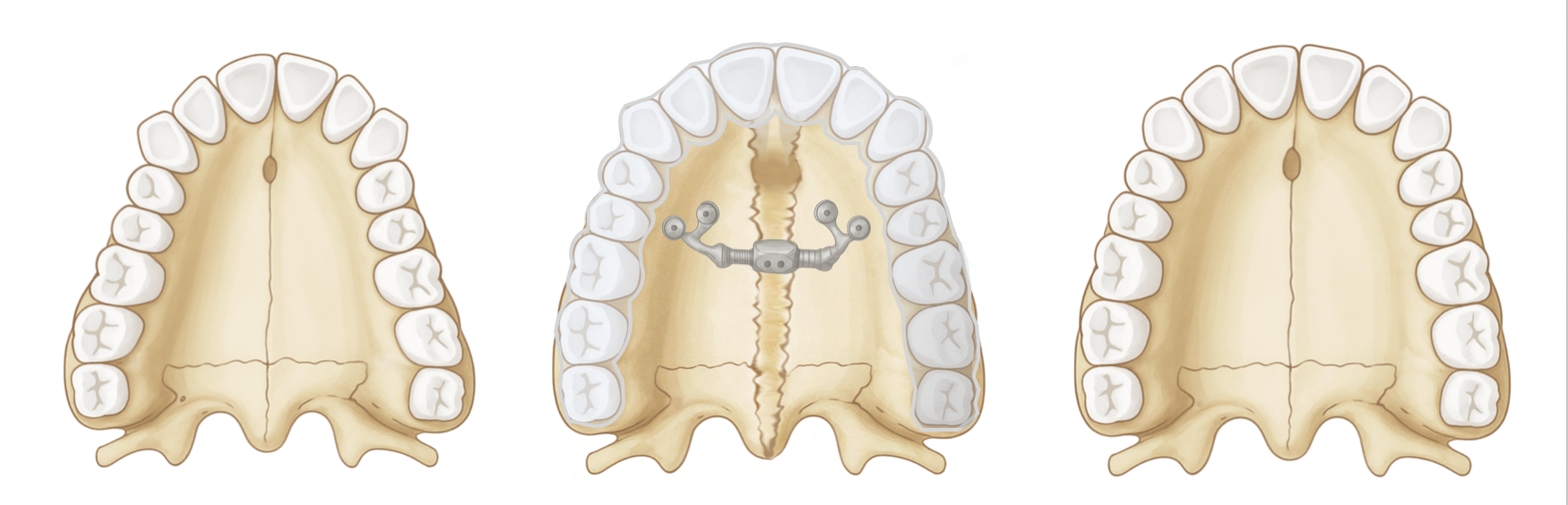
To open the palatal suture in adults, more force and time are required. A mini-implant supported expander makes this possible. Instead of using the teeth as anchors, the force is transferred directly to the upper jaw bone via mini-screws. According to expert opinion, activation should be slow – moving away from Rapid Palatal Expansion (RPE, MARPE) towards Slow Palatal Expansion (MASPE) to best avoid complications.

Custom-made 4 mini-implant supported expander.
Teeth can be included as additional anchors in the appliance (e.g., MSE), but this does not only bring advantages. The teeth can be moved out of the bone and cause discomfort – especially if the skeletal expansion does not work as planned.

Teeth can be included as additional anchors in the appliance, but this does not only bring advantages.
What do you do if skeletal upper jaw expansion with mini-implants does not work?
If the resistance to expansion is too great, bone cuts can be helpful. Here, too, there are various approaches (SARPE, SABAME, DOME, MISMARPE, Le-Fort I osteotomies …).
What they have in common: All techniques involve bone cuts in the upper jaw to reduce resistance and enable skeletal expansion.
How they differ: in the extent of the cuts.
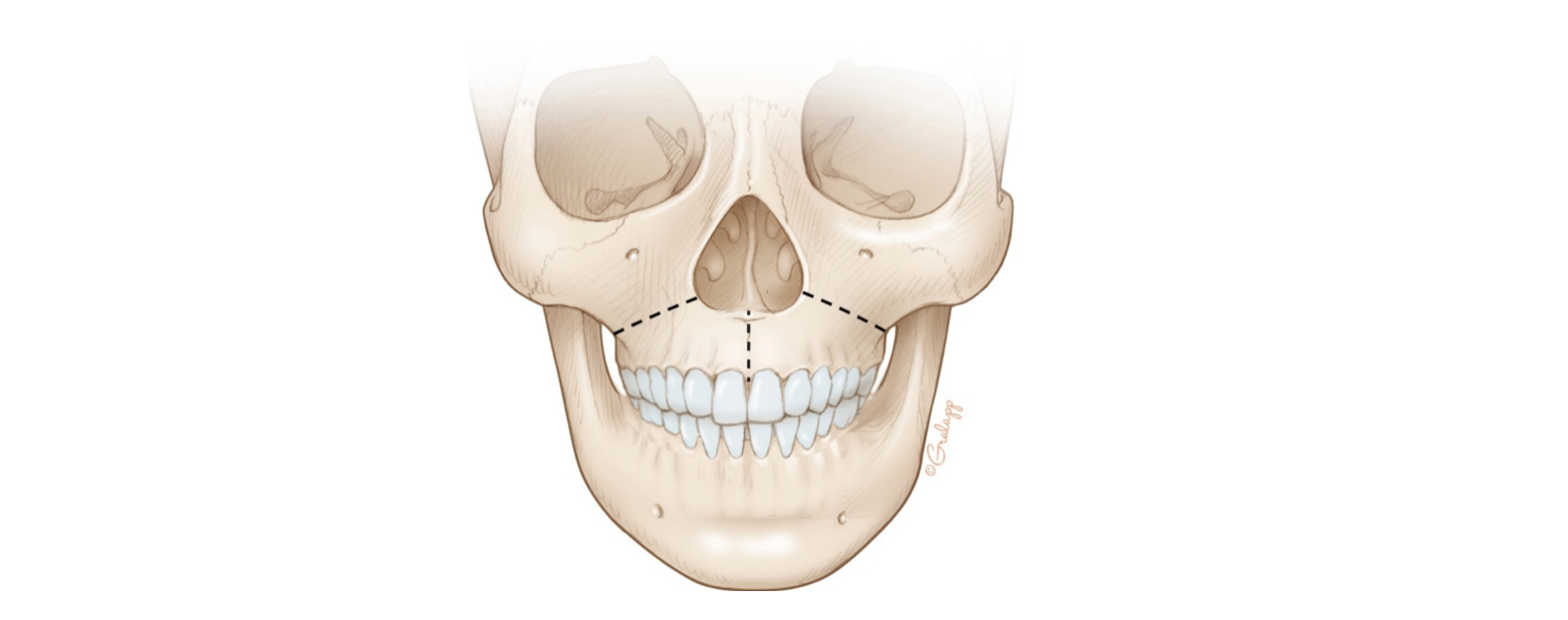
The dashed lines mark the osteotomies (bone cuts) that facilitate upper jaw expansion.
Generally, the more extensive the cuts, the higher the probability of success – but invasiveness also increases simultaneously.
Who additionally benefits from bone cuts and for whom expansion works without them cannot yet be reliably predicted. However, experts agree that it works better without surgical cuts in women than in men, and better in younger individuals than in older ones.
In summary, MARPE, MASPE, MSE, SARPE, etc., all refer to techniques that skeletally expand the upper jaw.
I am convinced that treatment should be tailored to the individual needs and circumstances of the patient. Therefore, I like to use the term DOME. According to the author of this concept, Dr. Stanley Liu, DOME prioritizes the outcome for the patient – not the technique. It means transforming a high, narrow palate into a functional, dome-shaped palate that provides enough space for the tongue and enables improved nasal breathing.
The latest development of this concept is DOMExD: While the upper jaw is slowly expanded, the teeth are simultaneously moved towards each other to prevent a bothersome gap from forming. The credit for this ingenious idea goes to Dr. Christian Leonhardt.
DOMExD: Upper jaw expansion for improved nasal breathing and more tongue space without a tooth gap.